Systemic Changes To Address Racial Inequality: Part 7: Health Care
Systemic Changes To Address Racial Inequality in Health Care
One of saddest health statistics in our country is about infant mortality and race. For White Americans there are 4.9 deaths per 1,000, while for Black Americans there are 11.4 deaths per 1,000. That disparity represents a total per year of 3,770 Black children who die at birth more than if the infant mortality rate was the same for White children. These stark disparities could be a reflection of a greater percentage of Black Americans living in poverty. This is another area where solving economics will alleviate a lot of the current problems.
Anti Bias Training: Although poverty may be a leading cause of the infant mortality disperity, bias may also play a role. Anti bias training in medical school and in hospitals could help bridge this gap. From the article Black doctors push for anti-bias training in medicine to combat health inequality by CNBC:
“We need to start in the medical school. There need to be lectures on social determinants of health, lectures and training and study on implicit bias,” said Harris, recalling her own course material when she trained to be a doctor. “When you learn about burns and rashes and skin diseases, they are described in white patients.”
“Research has shown that for patients of color this lack of diversity can translate into less-responsive care. Black patients are generally undertreated for pain than are White patients, according to a 2016 study that found White medical students and residents believed the Black body was “biologically different — and in many cases, stronger — than the White body,” and in some cases believe that Blacks have a higher tolerance for pain.”
The Affordable Care Act: Our healthcare system is a mess. Earlier I talked about how our government assistance programs created disincentives to work, well our current healthcare system has a major one. Under Obamacare there are several drop offs where earning $1 more can cost thousands of dollars in subsidies, most notably at 400% of the federal poverty line. We need to eliminate these drop offs, which cause confusion, loss of coverage, and extreme increases in health care costs.
Our healthcare system also has a major disconnect between who receives care and who pays for it (typically the government or insurance companies), allowing for runaway costs. These proposals will not fix everything wrong with our healthcare system, but they could make a dent in it.
Insurance Negotiated Rates for All: The main benefit to having health insurance for the most part isn’t even the amount of money they are supposed to pay, its the discounts they receive from healthcare providers. If cash patients received the same pricing as insured patients the economic toll of going to the hospital would not be so large. What other business operates like this? “Oh, you are a customer of a company that does a lot of business with us, here, let’s reduce your price by 70%.” In any other industry you may see a 5% to 15% reduction, but 70%?
Transparency in Service Pricing Before Services Rendered: I hate that you have no idea how much a visit to the hospital is going to cost, sometimes you can’t even guess how many digits the bill will be. When people know what the pricing is they can shop around and attempt to negotiate for lower pricing.
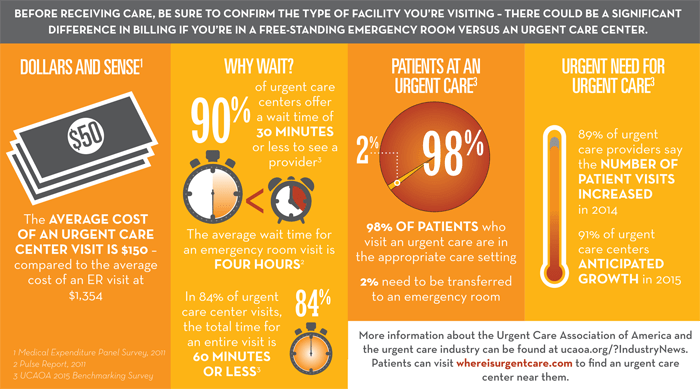
More Urgent Care Clinics: Urgent care clinics perform an important service and cost way less than an Emergency room visit. The average visit to an urgent care clinic costs around 10% of a visit to the ER. They also alleviate the strain emergency rooms face by taking care of patients who are not facing a life threatening situation.
Repeal ALL Certificate of Need Laws: Certificate of need laws have created a monopoly for hospitals, costing patients thousands of dollars. In 1 example, Dr. Singh in North Carolina has had to file suit to be able to buy an MRI machine and offer imaging services at his office for typically under 25% of what the hospital charges. These same laws also drive up the cost of ambulance services and other routine medical exams and treatments.
Support Medial Debt Relief: Medical debt is a factor in the majority of bankruptcies in this country. RIP Medical Debt buys debt on the open debt market in bulk quantities for around 1 cent on the dollar. They then forgive this debt, which results in no tax liabilities or negative consequences for the people who owed the money. So far RIP Medical Debt has paid off over 1.5 BILLION of medical bills. Ever $1 donated to RIP Medical Debt pays off $100 in past medical bills for low income Americans, which in addition to reducing economic strain will also in the long term help raise credit scores, making home ownership easier.
More Doctors:
We have a lack of primary care physicians in this country and are facing a major shortage of virtually all medical professionals in the US as the baby boomer population ages. The medical professionals we have are more likely to respond to financial incentives to work in higher income neighborhoods. By 2032 we will have a shortage of over 100,000 physicians.
Becoming a doctor has an extremely high barrier to entry. It requires a minimum of 11 years of schooling (including residency). This schooling in addition to being expensive also carries with it a major opportunity cost of years where the future doctor is in school instead of working. To get more doctors we need to reduce the barriers to becoming a doctor.
“Solutions to this problem are clear: decrease total cost of tuition, decrease hidden expenses, decrease total time of medical education, decrease interest rate impact, reenact subsidized loans, or enhance or front load repayment.” -Aaron George DO; Medical Economics
If we lower the cost to become a doctor we will have more doctors. If we have more doctors then supply and demand will dictate that more doctors will serve in areas that have been underserved. This will increase the supply of doctors in low income, Black neighborhoods.
Encouraging More Black Kids To Become Doctors:
My family doctor, Doctor Tynes, based in Benton Harbor, MI runs a program called “Future Doctor’s Future Leaders” designed to help kids become interested in becoming doctors. I think coupled with the economic solutions mentioned above programs like this can greatly increase the number of Black children who become doctors.
Please check out this article on Having a Black Doctor Led Black Men to Receive More-Effective Care
Black patients in particular have among the worst health outcomes, experiencing higher rates of hypertension and stroke. And black men have the lowest life expectancy of any demographic group, living on average 4.5 fewer years than white men. A number of factors contribute to these health disparities, but one problem has been a lack of diversity among physicians. African Americans make up 13% of the U.S. population, but only 4% of U.S. doctors and less than 7% of U.S. medical students. Research has found that physicians of color are more likely to treat minority patients and practice in underserved communities. And it has been argued that sharing a racial or cultural background with one’s doctor helps promote communication and trust.
They found that black men seen by black doctors agreed to more, and more invasive, preventive services than those seen by nonblack doctors. And this effect seemed to be driven by better communication and more trust. Increasing demand for preventive care could go a long way toward improving health. A substantial part of the difference in life expectancy between white and black men is due to chronic diseases that are amenable to prevention. By encouraging more preventative screenings, the researchers calculate, a workforce with more black doctors could help reduce cardiovascular mortality by 16 deaths per 100,000 per year — resulting in a 19% reduction in the black-white male gap in cardiovascular mortality and an 8% decline in the black-white male life expectancy gap.
Check out this article titled “Why We Need More Black Doctors”
“Our nation needs more black doctors, especially black male doctors.
Why? Because the talents of young black men who would make outstanding doctors are being wasted since so few make it into the medical profession and because black people need far greater access to culturally connected physicians who understand their lives and their challenges as much as their clinical needs.
A little more than a year ago, the Association of American Medical Colleges sounded the alarm, reporting that there were fewer black males applying to and attending medical school than in 1978 — this in a nation that doesn’t have doctors to spare and whose minority population has ballooned over the last 40 years.”
I know for this article I used a lot of quotes. I wanted to get the point across and the articles I referenced did a better job of putting the ideas into words than what I could. My goal is to spread information and get people thinking. If your gears are turning then I did my job.
Actions You Can Take:
- Encourage your employer to offer anti-bias training
- Insist on seeing a price list before accepting medical care (except in an emergency situation). Even if you are paying through insurance. The more people request pricing the more likely it is that medical providers will publish it.
- Contact your congressman and senators about enacting policies to make medical school more affordable and at the state level to throw out certificate of need laws.
- Encourage kids in your life to pursue a career in medicine.
- Donate to RIP Medical Debt. Bonus: Check to see if your employer matches, then every $1 donated would forgive $200 of medical debt!
Leave a Reply